1 Why health data is different
Health data is different because it mirrors the complexity of healthcare itself: it is multimodal, longitudinal, and deeply human. It spans everything from demographics and vitals to labs, imaging, genomics, medications, pathology, clinical narratives, and social determinants, yet it is often fragmented across organizations and trapped in semi-structured, unstructured, or even paper formats. This complexity makes the field intimidating for newcomers and raises the stakes for getting things right. The chapter frames a unifying model for safe, effective care built on two pillars—precision (technical correctness and timeliness) and trust (privacy, security, and governance). When these align, data supports timely decisions at the point of care; when they do not, patient safety and outcomes are at risk.
The text details how disconnected systems and inconsistent implementations undermine reliable exchange, creating silos and risking errors. It argues that precision is foundational, operationalized through rigorous handling of identity, timestamps, provenance, semantics, governance, privacy, security, storage, interoperability, and analytics—because small lapses can cascade into adverse events, repeat scans, delayed treatments, and even avoidable deaths. Equally essential is trust, grounded in a regulatory lineage that transforms statutes into developer-facing requirements: HIPAA’s statutory origins, the pathway from law to rules and codified regulations, and the complementary scope of the Privacy Rule (when and why PHI may be used) and the Security Rule (how ePHI must be protected). Together, these frameworks turn ethical obligations into concrete design constraints that shape health IT systems.
Tracing the policy arc from 1996 to the present, the chapter shows how national priorities drove digitization and interoperability: ONC’s establishment and strategy, HITECH’s incentives and certification that catalyzed EHR adoption, and the 21st Century Cures Act’s push against information blocking and toward standardized, patient- and provider-facing APIs. With growing adoption and maturing APIs, initiatives like TEFCA and efforts to replace paper workflows signal a shift from mere compliance to value creation and better experiences. Yet the chapter cautions that success depends on integrating technology into real clinical workflows and honoring both pillars—highlighted by lessons from high-profile failures that neglected precision, context, or user trust. For developers, the mandate is clear: build within evolving technical and regulatory frameworks, center patient safety and privacy, and treat precision and trust as the core architecture of systems that can scale, interoperate, and ultimately save lives.
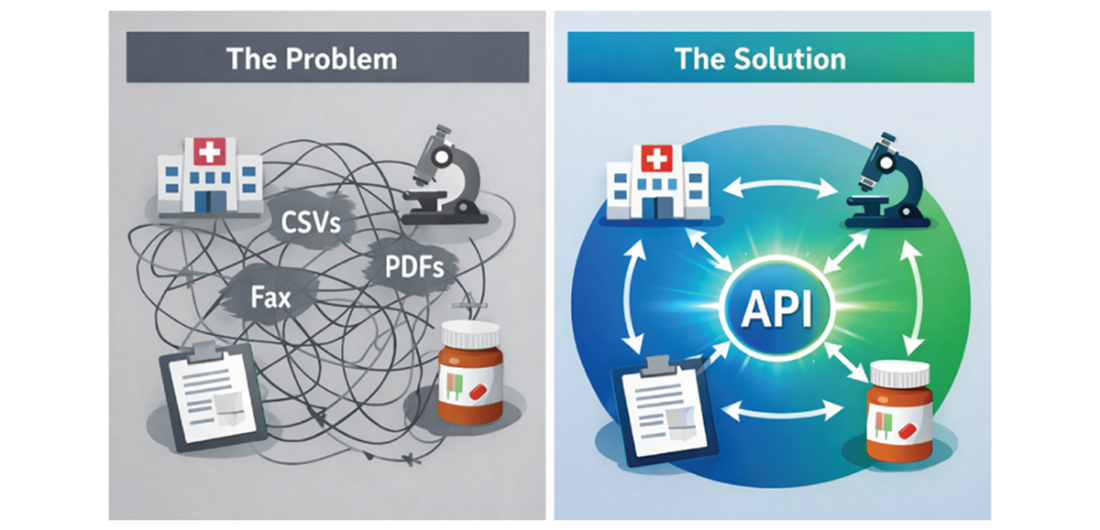
The day-to-day reality: fragmented systems exchanging data as files and faxes—versus clean, bidirectional exchange through APIs.
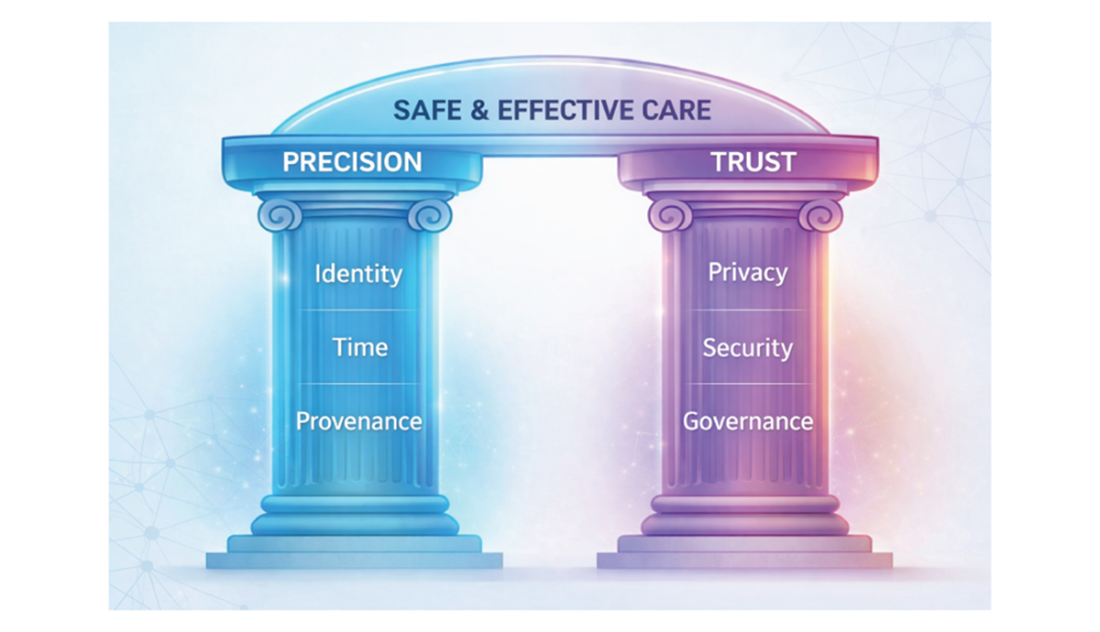
“Precision“(technical correctness) and “trust“ (regulatory/operational safeguards) are the pillars of safe, effective care.
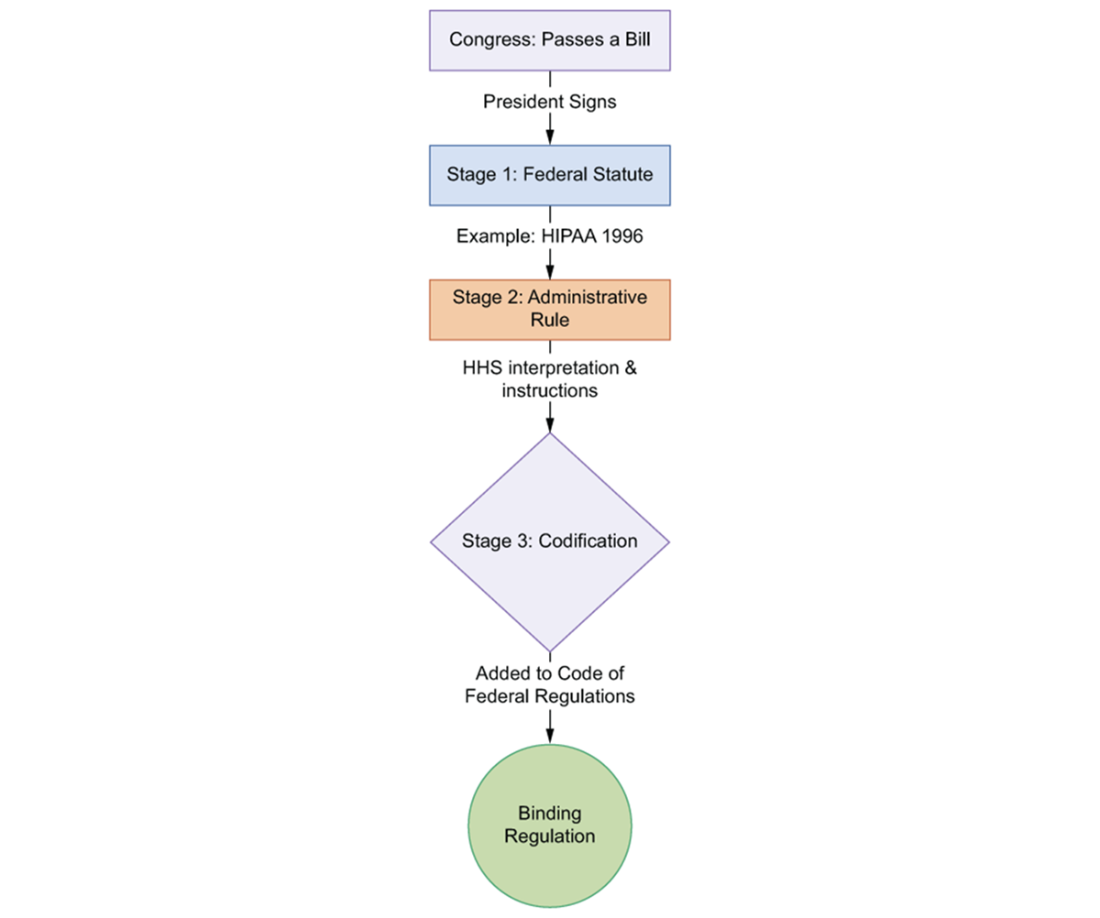
How a law becomes developer-facing requirements: Statute → Administrative Rule → Codified Regulation.
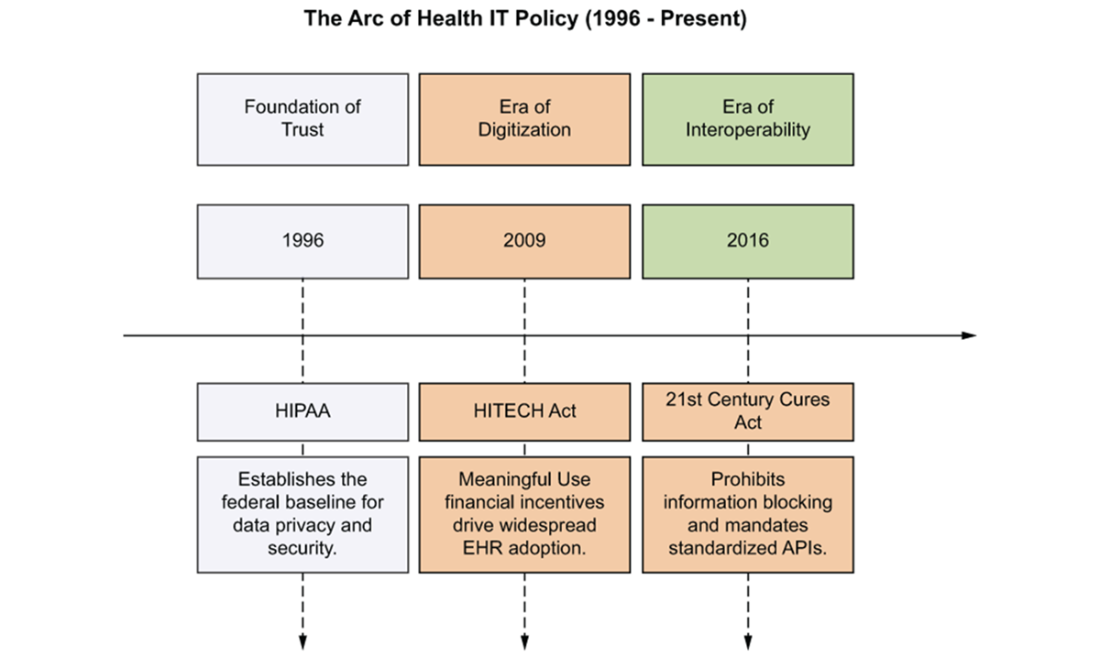
The progression of U.S. health IT policy: Trust baseline → Digitization incentives → Interoperability mandates.
Summary
- Health data is fundamentally different from data in other industries because it is longitudinal, multimodal, and directly tied to human lives, making errors both technical and clinical risks.
- Healthcare software must balance two inseparable pillars: precision and trust. Precision ensures data is technically correct and usable at the point of care, while trust ensures privacy, security, and regulatory compliance.
- Fragmentation is the central challenge of modern health IT. Clinical information exists across many systems, formats, and organizations, requiring interoperability rather than isolated applications.
- Every technical decision in health IT carries patient-safety implications. Issues such as identity matching, timestamps, provenance, terminology, and governance directly affect clinical outcomes.
- Regulation shaped modern health IT architecture. HIPAA established privacy and security expectations, HITECH accelerated digitization through EHR adoption, and the 21st Century Cures Act pushed the industry toward interoperable, API-driven systems.
- Healthcare is transitioning from document exchange to data exchange. The industry is moving away from files, faxes, and siloed systems toward standardized, real-time data sharing.
 Healthcare IT ebook for free
Healthcare IT ebook for free